Key takeaways
Non-identical (fraternal) twins are the most common and usually have the lowest pregnancy risk
Identical twins can share or have separate placentas and sacs, which changes monitoring and risk
Only non-identical twins usually run in families on the mother’s side
A simple home cheek swab zygosity test can confirm if twins are genetically identical
If you’ve just found out you’re expecting twins, one of the first questions that may come to mind is, ‘are my twins identical or non-identical?’
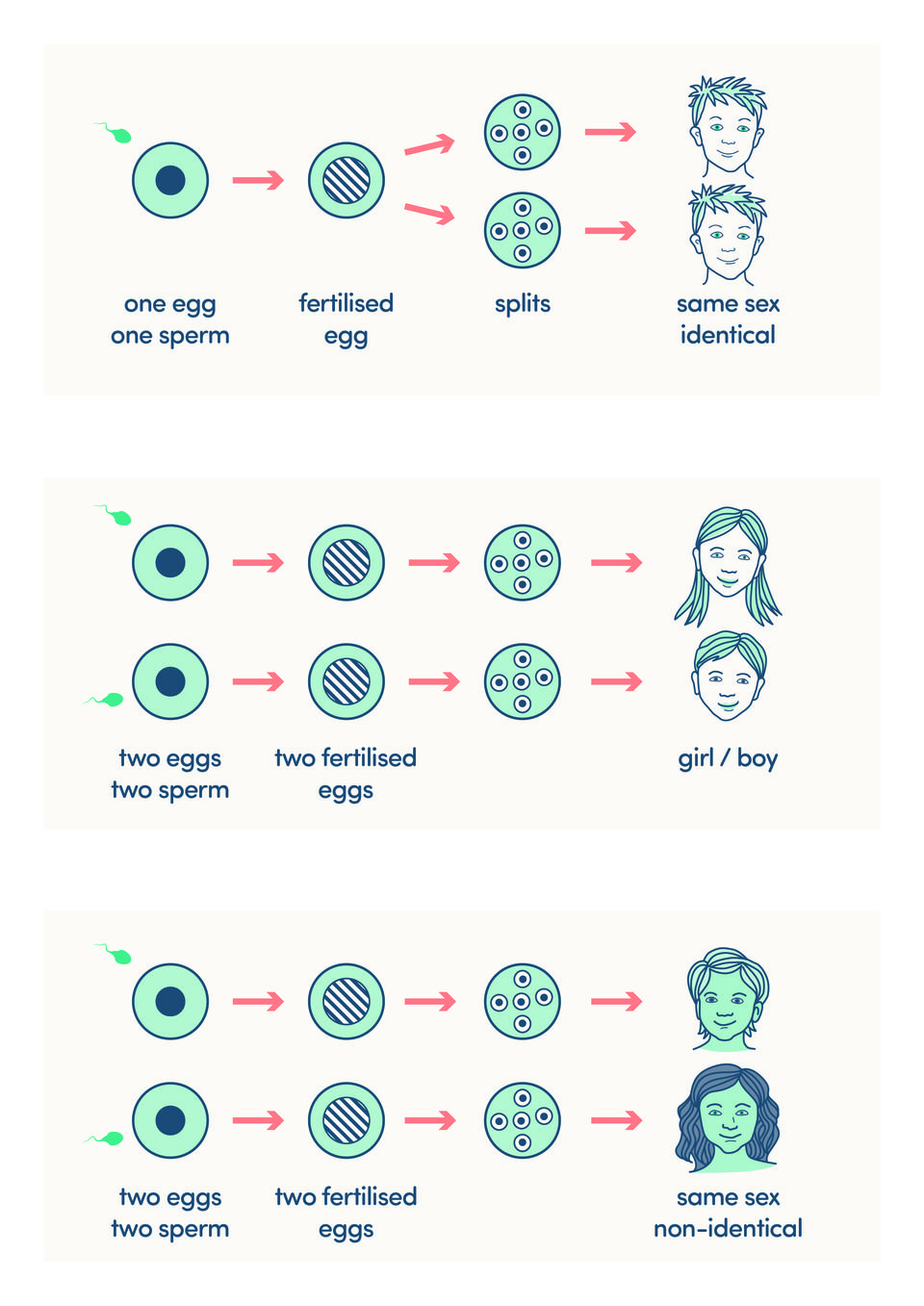
There are two main types of twins. Identical twins are known medically as monozygotic. Non-identical, or fraternal, twins are called dizygotic. Understanding these terms can help you make sense of what your sonographer and midwife explain.
Identical twins come from a single egg and a single sperm. After fertilisation, the egg splits into two embryos. They share the same genetic make-up, are always the same sex and usually look very similar.
Non-identical twins come from two separate eggs and two separate sperm. They share around half their genes, like any other siblings. They can be different sexes and may not look any more alike than brothers or sisters born at different times.
In this article we look at how twin pregnancy types affect your care, how family history plays a role and how you can confirm whether twins are identical.
How twin pregnancy types affect your care
At around 12 weeks, your ultrasound scan should confirm that you are carrying twins. The sonographer will check whether your babies share a placenta and whether they share an amniotic sac. It is not possible for twins to share a sac without also sharing a placenta.
There are three main twin pregnancy types:
Dichorionic diamniotic (Di/Di) twins each have their own placenta and their own amniotic sac
Monochorionic diamniotic (Mo/Di) twins share a placenta but have separate sacs
Monochorionic monoamniotic (Mo/Mo) twins share both a placenta and a sac
Di/Di twins can be either identical or non-identical. Mo/Di and Mo/Mo twins are always identical.
The type of pregnancy changes the level of risk and how often you are seen. Twins with their own placenta and sac (Di/Di) usually have the lowest risk of complications. When twins share a placenta (Mo/Di), the risk is higher, so you will be offered more frequent scans. Mo/Mo twins have the highest risk and are monitored very closely.
In the UK, about one in 65 pregnancies results in a twin birth. Every pregnancy has about a one in 250 chance of resulting in identical twins. Identical twins are thought to happen as a random event when one fertilised egg splits in two, rather than because of family history.
Genetics, family history and testing for twin type
People often ask parents of twins, ‘does it run in the family?’ Only non-identical twins are usually hereditary, and this is on the mother’s side. This is because some women are more likely to release more than one egg during ovulation.
Factors that can make non-identical twins more likely include:
- Fertility treatment such as IVF where more than one embryo is transferred
- Maternal family history of non-identical twins
- Being over 35 when you conceive
- Some ethnic backgrounds, with higher rates in Nigerians and lower in Japanese people
Identical twins do not seem to be linked to these factors. They happen when a fertilised egg divides into two embryos.
Even though identical twins share all their DNA, you will still notice differences. Weight can vary, both in the womb and after birth. They will have different fingerprints. Birthmarks, freckles, teeth and bite pattern can differ. Most of all, their personalities and interests will develop in their own unique ways.
If you are unsure whether your twins are identical, especially after a Di/Di pregnancy, you can choose a zygosity test. This uses cheek swabs from each twin to collect DNA cells. The test is painless, can be done at any age and is simple to carry out at home by following the kit instructions.
How to find out if twins are genetically identical
If you want to know whether your twins are genetically identical, a DNA test can give you a clear answer. During a zygosity test, a lab takes a small sample of cheek cell DNA from each person using a cheek (buccal) swab. It's non-invasive and painless, so it can be done at any age, from birth to adulthood.
Twins Trust Premium Members can save 10% on zygosity tests from AlphaBiolabs or NorthGene. Join today to claim this saving and much more.
Feeling supported as you prepare for life with twins
Knowing whether your twins are identical or non-identical can help you understand your scan results, your care plan and those frequent questions about twins ‘running in the family’.
Your midwife, sonographer and doctor are there to explain any terms you are unsure about. If you do not understand what type of twin pregnancy you have, or what that means, it is always okay to ask again.
Whether your twins share all their genes or only some of them, each child will grow into their own person. Understanding your twin pregnancy type, and knowing there is support available, can help you feel more confident and prepared as you get ready to welcome your children.
Feel prepared for life with twins
Expecting twins? Get practical, bite-sized guidance plus access to an interactive drop-in session where you can ask questions, with our Preparing for twins on-demand course.